Description
This is the more clinical information. For the personal stories, please visit the People page.
Carpenter Syndrome belongs to a group of genetic disorders known as Acrocephalopolysyndactyly, Type II (pronounced: AK-roh-SEF-ah-loh-PAH-lee-sin-DAK-tuh-lee) or ACPS disorders. All forms of ACPS are characterized by webbing or fusion (syndactyly) of certain fingers and/or toes (digits), more than the expected number of digits (polydactyly), and by the premature closure of the fibrous joints (cranial sutures) between certain bones of the skull, which is known as craniosynostosis and causes the top of the head to appear pointed or cone shaped (acrocephaly).
|
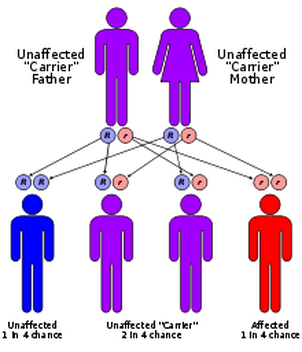
With an estimated occurrence rate of one in one million live births, people with Carpenter Syndrome really are one in a million! Currently, there are approximately 300 million people in the U.S., which means there should be about 300 cases (but we only know of FIVE!) in the entire country! Carpenter Syndrome is an inherited autosomal recessive trait. The odds of two people who unwittingly carry the defective gene, meeting and reproducing, are astronomical. Each biological parent carries a copy (or two if they have Carpenter Syndrome, themselves) of the affected gene. When two carriers procreate, each has a 50/50 chance of passing on the affected gene to the child. With each pregnancy created by
|
two carriers, there is a 25% chance the baby will have Carpenter's Syndrome. A 50% chance the baby will be a carrier, but unaffected themselves, and a 25% chance the child will inherit "normal" copies of gene from each parent (and be completely unaffected), and ending the cycle. A person who has Carpenter Syndrome has inherited a copy of the defective gene from each of their biological parents. Since they don't have a "normal" copy of that particular gene, they will pass it on to any offspring they produce. However, unless their mate also carries a copy of this particular gene, their children will be carriers, but otherwise unaffected.
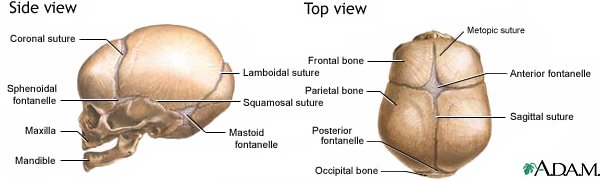
A level 2 ultrasound is often done during pregnancy if fetal abnormalities are suspected. More often in the case of Carpenter Syndrome, it seems the first sign of anything out of the ordinary, is the craniosynostosis which is obvious at birth. Craniosynostosis is a medical term which literally means "fused bones of the skull". The premature fusion of the cranial sutures cause the skull to grow abnormally. Depending on which sutures are involved, the skull, most commonly, will have either a short (front to back) "cloverleaf" shape (brachycephaly), or a pointed "cone" shape (acrocephaly).
Common differences of the facial region includes epicanthal folds ("oriental" looking eye); broad cheeks; low set, uneven, and often malformed ears; small, widely spaced teeth that may be late to erupt (and come out); flat nasal bridge; wide upturned nose with large nasal openings; an underdeveloped maxilla and/or mandible; and a highly arched and narrow palate which can make speech difficult and contribute to sometimes severe oral aversion and defensiveness.
Other physical characteristics associated with Carpenter Syndrome are polydactyly (extra digits); syndactyly (webbed or fused digits); brachydactyly (unusually short fingers, often with just a single joint in each) which interestingly, have begun to develop before the 6th gestational week. There are heart defects in about half of the known cases. A single horseshoe shaped kidney, rather than two separate ones, undescended testes in the males, abdominal hernias, and rocker bottom feet are also not uncommon.
Mild to moderate mental deficiencies should be anticipated (about 75% of all cases), but are not an obligate feature. A short, stock stature is also common because of the shortened proximal long bones of the upper arms and legs (which at birth, is sometimes mistaken for non-proportional dwarfism).
A level 2 ultrasound is often done during pregnancy if fetal abnormalities are suspected. More often in the case of Carpenter Syndrome, it seems the first sign of anything out of the ordinary, is the craniosynostosis which is obvious at birth. Craniosynostosis is a medical term which literally means "fused bones of the skull". The premature fusion of the cranial sutures cause the skull to grow abnormally. Depending on which sutures are involved, the skull, most commonly, will have either a short (front to back) "cloverleaf" shape (brachycephaly), or a pointed "cone" shape (acrocephaly).
Common differences of the facial region includes epicanthal folds ("oriental" looking eye); broad cheeks; low set, uneven, and often malformed ears; small, widely spaced teeth that may be late to erupt (and come out); flat nasal bridge; wide upturned nose with large nasal openings; an underdeveloped maxilla and/or mandible; and a highly arched and narrow palate which can make speech difficult and contribute to sometimes severe oral aversion and defensiveness.
Other physical characteristics associated with Carpenter Syndrome are polydactyly (extra digits); syndactyly (webbed or fused digits); brachydactyly (unusually short fingers, often with just a single joint in each) which interestingly, have begun to develop before the 6th gestational week. There are heart defects in about half of the known cases. A single horseshoe shaped kidney, rather than two separate ones, undescended testes in the males, abdominal hernias, and rocker bottom feet are also not uncommon.
Mild to moderate mental deficiencies should be anticipated (about 75% of all cases), but are not an obligate feature. A short, stock stature is also common because of the shortened proximal long bones of the upper arms and legs (which at birth, is sometimes mistaken for non-proportional dwarfism).
What is Craniosynostosis?
The Jorge Posada Foundation has a lot of great information and images that will help this condition make a little more sense.
New Information on the Genetics
RAB23 mutation in a large family from Comoros Islands with Carpenter syndrome.
NORD
National Organization for Rare Disorders, Inc. offers some in depth information on Carpenter Syndrome.
